Exposure and Response Prevention (ERP) is one of the most extensively researched psychological treatments for OCD and is recommended within international clinical guidelines for individuals experiencing symptoms of OCD.
More recently, Inference-Based Cognitive Behavioural Therapy (I-CBT) has emerged as another evidence-based treatment option and has attracted growing interest among clinicians and individuals living with OCD. The growing body of evidence for I-CBT has contributed to growing confidence in delivering this approach.
For someone seeking OCD treatment options, this naturally raises questions. Is I-CBT simply another version of ERP? Is it an alternative to exposure therapy? Is one approach better than the other? And how do psychologists determine which treatment may be the best fit for a particular individual?
The answer is often more nuanced than many people expect.
Although ERP and I-CBT conceptualize OCD differently and use somewhat different therapeutic strategies, both approaches share the same overarching goal: helping individuals reduce compulsions, disengage from the OCD cycle, and regain greater freedom in their lives.
Rather than viewing ERP and I-CBT as competing therapies, it is often more helpful to think of them as two evidence-based approaches that understand OCD differently while ultimately working toward the same goal for the client.
This article explains how ERP and I-CBT compare, what current research tells us about each approach, and how psychologists think about selecting the treatment that may be the best fit for an individual’s needs.
What is the difference between ERP and I-CBT?
ERP and I-CBT are both evidence-based treatments for OCD, but they differ in how they understand the development and maintenance of OCD symptoms.
ERP conceptualizes OCD as a condition in which intrusive thoughts or feared situations trigger distress and lead to compulsions or avoidance behaviours that temporarily reduce anxiety. Unfortunately, this relief reinforces the OCD cycle over time. Therapy for OCD, therefore, focuses on gradually approaching feared situations, thoughts, images, or sensations while reducing compulsive responses. Through repeated experiences, individuals develop new learning, strengthen their ability to tolerate distress, and discover that compulsions are unnecessary.
I-CBT begins from a different conceptual framework. Rather than focusing primarily on what happens after an obsession occurs, I-CBT examines the reasoning process that allowed obsessional doubt to develop in the first place. The therapy helps individuals recognize inferential confusion. We can understand this as the moment when imagination begins to replace direct sensory information and reality-based evidence. I-CBT interventions support individuals in reconnecting with reality before compulsions become necessary.
Although these conceptualizations differ, the therapies share an important goal. Both ultimately help individuals disengage from OCD by reducing compulsions and interrupting the processes that keep the disorder going.
Why do both therapies work if they seem so different?
Although ERP and I-CBT take different therapeutic paths, both are supported by research demonstrating their effectiveness in treating OCD.
At first glance, the therapies may appear quite different. ERP encourages individuals to gradually approach feared situations while reducing compulsions. I-CBT focuses on helping individuals understand and modify the obsessional reasoning process that gives rise to doubt before compulsions occur.
However, both therapies ultimately aim to weaken OCD’s influence over everyday life.
In clinical practice, psychologists are often less interested in whether two therapies use identical techniques and more interested in whether they help individuals disengage from the processes that maintain OCD. ERP and I-CBT approach this objective differently, but both seek to reduce reliance on compulsions and help individuals respond to OCD in healthier, more adaptive ways.
Rather than asking which therapy is universally “better,” a more clinically useful question is often which evidence-based approach may be the best fit for a particular individual.
What is each therapy trying to change?
One of the clearest ways to understand ERP and I-CBT is to consider the primary therapeutic target of each approach.
ERP primarily targets the compulsive behaviours and avoidance patterns that maintain OCD. By reducing compulsions while gradually approaching feared situations, individuals have opportunities to develop new learning, build confidence in their ability to tolerate distress, and discover that compulsions are not required to remain safe.
I-CBT targets a different point within the OCD cycle. Rather than beginning with exposure, it focuses on the inferential confusion and obsessional reasoning that lead an individual to doubt what they know through direct experience. Treatment helps individuals recognize when OCD has pulled them away from reality-based information and into imagined possibilities.
Although these therapeutic targets differ, the ultimate destination is remarkably similar. Both therapies seek to reduce compulsions, increase psychological flexibility, and help individuals live more fully according to their values rather than according to OCD.
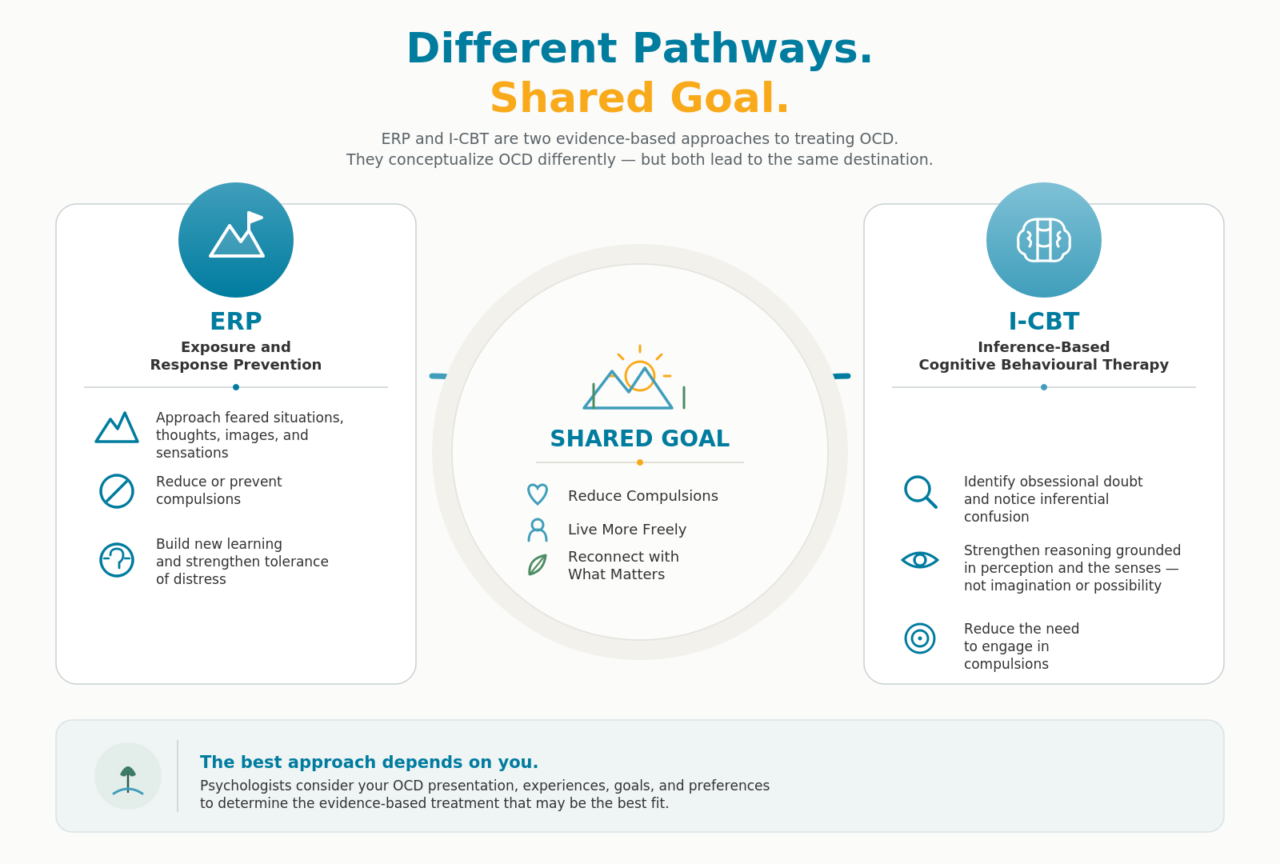
Figure 1. ERP and I-CBT take different evidence-based pathways toward the shared goal of reducing compulsions and helping individuals regain freedom from OCD.
Is I-CBT an alternative to ERP?
Yes. I-CBT is an evidence-based psychological treatment for OCD and is considered an alternative to ERP for many individuals.
Describing I-CBT as an “alternative,” however, does not mean that one therapy has replaced the other. It also does not mean that I-CBT for OCD is only delivered after ERP has been used as an intervention. Many individuals want to engage in I-CBT for OCD at the start of their treatment.
It is important to note that ERP remains one of the most extensively researched psychological treatments for OCD and continues to be delivered by numerous mental healthcare professionals.
At the same time, research supporting I-CBT has expanded considerably over the past two decades. Multiple randomized controlled trials and systematic reviews now support I-CBT as an evidence-based treatment for OCD, although the research base remains smaller than that of ERP.
For some individuals, I-CBT’s emphasis on understanding obsessional reasoning resonates strongly with how they experience OCD and may feel like a better therapeutic fit.
In practice, the decision is rarely based on whether one therapy is objectively superior. Instead, psychologists and other mental health professionals should consider the individual’s OCD presentation, treatment history, preferences, goals, and the clinical formulation developed during assessment before recommending a treatment approach.
Does research suggest that one therapy is more effective than the other?
Current research suggests that both ERP and I-CBT are effective treatments for OCD, although the evidence base for each differs in size and maturity.
ERP has been studied for several decades, and its effectiveness has been demonstrated across numerous randomized controlled trials, clinical settings, and age groups. It is used throughout the world in both outpatient and inpatient settings.
Research supporting I-CBT has grown considerably over the past two decades. Multiple randomized controlled trials have demonstrated that I-CBT can significantly reduce OCD symptoms, with several studies suggesting outcomes that are comparable to ERP for many individuals.
Current comparative studies suggest that both therapies can produce meaningful reductions in OCD symptoms. However, further research will continue to clarify whether particular individuals or OCD presentations benefit more from one approach than another.
In clinical practice, psychologists recognize that research provides important guidance, but it cannot determine the best treatment for every individual. Two people with OCD may present very differently, respond differently to therapy approaches, or find that one therapeutic model resonates more strongly with how they experience OCD. This is one reason why individual treatment recommendations are based not only on research findings but also on comprehensive assessment, clinical formulation, and collaborative decision-making.
It is also important to recognize that research comparing psychological therapies is inherently complex. Individuals seeking treatment differ in the types of OCD they experience, the severity of symptoms, previous treatment experiences, and other factors that may influence outcomes. While randomized controlled trials provide valuable information about effectiveness, they cannot determine which therapy will be the best fit for every individual. This is one reason why clinical expertise and collaborative decision-making remain important parts of treatment planning.
Who might benefit more from ERP or I-CBT?
There is no simple formula for determining which evidence-based therapy is the best fit for an individual with OCD.
Some individuals appreciate ERP’s behavioural approach and find that gradually approaching feared situations while reducing compulsions helps them develop confidence in their ability to tolerate distress and respond differently to OCD. Others describe feeling that I-CBT provides a framework that more closely matches their own experience of obsessional doubt, particularly when they recognize how imagination and inferential confusion contribute to their OCD.
Importantly, these observations should not be interpreted as strict rules. Individual preferences, previous treatment experiences, symptom presentation, motivation, and therapeutic rapport all contribute to treatment planning. The same diagnosis does not necessarily require the same treatment approach for every person.
Rather than asking which therapy people with OCD “should” receive, psychologists typically ask a different question:
Which evidence-based approach is most likely to help this individual achieve their treatment goals?
Can ERP and I-CBT be integrated?
Yes. Some clinicians with training in both approaches thoughtfully integrate elements of ERP and I-CBT when it is clinically appropriate to do so.
Although ERP and I-CBT are often presented as separate therapeutic models, the reality of clinical practice is frequently more nuanced. Both therapies are grounded in cognitive behavioural principles and share the ultimate goal of reducing compulsions and helping individuals disengage from OCD.
However, because these two approaches do hold different conceptualizations of OCD, clinicians must be well-versed in both interventions in order to truly understand what, if any, components might be combined within the same treatment journey.
For some individuals, treatment may primarily follow one model while drawing selectively from the other when doing so supports the overall clinical formulation. For example, helping an individual better understand the reasoning process that contributes to obsessional doubt may enhance their ability to engage in behavioural work. Likewise, behavioural experiments may reinforce insights developed through I-CBT interventions. Further, encouraging an individual to engage in values-based activities fits within both approaches as well.
In practice, thoughtful integration is not simply a matter of combining techniques. It requires a solid understanding of both theoretical models and a clear clinical rationale for why particular interventions are being used. The emphasis remains on developing a coherent treatment plan that is responsive to the individual’s presentation rather than rigidly adhering to one approach in every circumstance.
Integration should never mean abandoning the theoretical foundations of either approach. Rather, clinicians who are trained in both therapies may thoughtfully determine whether particular concepts or interventions support the individual’s overall formulation while maintaining a coherent treatment plan.
How do psychologists decide which treatment may be the best fit?
Choosing between ERP and I-CBT involves much more than selecting one therapy over another.
Psychologists consider many factors when developing a treatment recommendation, including the individual’s symptom presentation, developmental history, previous treatment experiences, personal preferences, goals for therapy, and the clinical formulation that emerges during assessment.
For some individuals, one therapeutic model may more closely align with how they understand and experience their symptoms of OCD. Others may have previously completed one form of treatment and wish to explore another evidence-based approach. Some individuals are simply looking for a therapist who can discuss both models and help them make an informed decision together.
In clinical practice, the goal is never to convince someone that one therapy is universally superior. Instead, psychologists seek to understand the individual’s unique presentation and recommend an evidence-based approach that is likely to provide the greatest opportunity for meaningful and lasting change.
When working with a client, choosing a treatment is rarely about deciding which therapy is “better.” It is about understanding the individual sitting in front of you and selecting an evidence-based approach that best fits how their OCD operates.
Conclusion
ERP and I-CBT represent two evidence-based approaches to treating OCD. Although they conceptualize OCD differently and use different therapeutic strategies, both ultimately share the same goal: helping individuals reduce compulsions, step out of the OCD cycle, and live more freely according to what matters most to them.
Rather than thinking about ERP and I-CBT as competing approaches, it may be more helpful to think of them as two evidence-based pathways that conceptualize OCD differently while working toward the same goal: helping individuals reduce compulsions and reclaim their lives from OCD.
Increasingly, OCD research is moving beyond asking whether one evidence-based therapy is universally superior to another and toward understanding which approaches are most effective for particular individuals. This reflects the reality of clinical practice, where treatment planning is individualized rather than one-size-fits-all.
If you are considering treatment for OCD and would like to better understand which evidence-based approach may be the best fit for you, working with a psychologist who is trained in both ERP and I-CBT can provide an opportunity to explore these options collaboratively and develop a treatment plan tailored to your individual needs.
At Forward Thinking Psychological Services®, our psychologists provide evidence-based treatment for OCD using ERP, I-CBT, or an individualized treatment plan informed by a comprehensive understanding of your presentation and goals. If you would like to learn more about our OCD services or schedule an initial consultation, we would be happy to discuss how we may be able to help.

FAQs:
DISCLAIMER: This content is meant for informational and educational purposes only. Only a licensed psychologist or psychiatrist can diagnose a mental health disorder. The content of this website is not meant to be a substitute for therapy. Visiting this website should not be considered to be equivalent to a relationship with FTPS. Mental health concerns should only be discussed in the context of providing professional services after the consent process has been completed with a qualified FTPS associate outside of our website.
Make FTPS a Google Preferred Source
If you found our blog helpful, you can ensure our latest evidence-based mental health insights, tools, and recovery strategies always appear at the top of your Google Search and AI Overviews.



